SARS-CoV-2/Influenza A+B/RSV/Adenovirus Antigen Combo Rapid Test
(Nasopharyngeal Swab)
| Principle | Chromatographic Immunoassay |
| Format | Cassette |
| Specimen | Nasopharyngeal Swab |
| Certificate | CE |
| Reading Time | 15 minutes |
| Pack | 20 T |
| Storage Temperature | 2-30°C |
| Shelf Life | 2 Years |
The SARS-CoV-2/Influenza A+B/RSV/Adenovirus Antigen Combo Rapid
Test (Nasopharyngeal Swab) is a rapid chromatographic immunoassay for
the qualitative detection of SARS-CoV-2 Nucleocapsid protein, Influenza A, Influenza B,
Respiratory Syncytial Virus(RSV) and Adenovirus antigens present in human nasopharynx.
For professional in vitro diagnostic use only.
INTENDED USE
The SARS-CoV-2/Influenza A+B/RSV/Adenovirus Antigen Combo Rapid
Test (Nasopharyngeal Swab) is a rapid chromatographic immunoassay for
the qualitative detection of SARS-CoV-2 Nucleocapsid protein, Influenza A, Influenza B,
Respiratory Syncytial Virus(RSV) and Adenovirus antigens in nasopharyngeal swab specimens
from individuals with suspected SARS-CoV-2/Influenza/RSV/Adenovirus infection in
conjunction with clinical presentation and the results of other laboratory tests.
Results are for the detection of SARS-CoV-2, Influenza A+B, RSV and
Adenovirus antigens. An antigen is generally detectable in upper respiratory specimens
during the acute phase of infection. Positive results indicate the presence of viral
antigens, but clinical correlation with patient history and other diagnostic information is necessary to
determine infection status.
Positive results do not rule out other bacterial/viral infection.
The agent detected may not be the definite cause of disease.
Negative results do not preclude SARS-CoV-2/Influenza
A+B/RSV/Adenovirus infection and should not be used as the sole basis for treatment or patient
management decisions. Negative results should be treated as presumptive and confirmed with a
molecular assay, if necessary for patient management. Negative results should be considered in
the context of a patient’s recent exposures, history and the presence of clinical signs and
symptoms consistent with SARS-CoV-2, Influenza A+B, RSV and Adenovirus.
SUMMARY
The novel coronaviruses belong to the β genus. COVID-19 is an acute
respiratory infectious disease. People are generally susceptible. Currently, the patients
infected by the novel coronavirus are the main source of infection; asymptomatic infected
people can also be an infectious source. Based on the current epidemiological
investigation, the incubation period is 1 to 14 days, mostly 3 to 7 days. The main manifestations include
fever, fatigue and dry cough.
Nasal congestion, runny nose, sore throat, myalgia and diarrhea are
found in a few cases. Influenza (commonly known as “flu”) is a highly contagious, acute
viral infection of the respiratory tract. It is a communicable disease easily transmitted
through the coughing and sneezing of aerosolized droplets containing live virus. Laboratory
identification of human influenza virus infections is commonly performed using direct
antigen detection, virus isolation in cell culture, or detection of influenza-specific RNA by reverse
transcriptase-polymerase chain reaction (RT-PCR). Rapid tests for influenza A and B virus
infections, which can provide
results within 30 minutes.
Respiratory Syncytial Virus (RSV), which causes infection of the
lungs and breathing passages, is a major cause of respiratory illness in young children. In
adults, it may only produce symptoms of a common cold, such as a stuffy or runny nose, sore
throat, mild headache, cough, fever, and a general feeling of being ill.Most children with
RSV infection, both those who were hospitalized and those who were treated as outpatients,
had no coexisting medical conditions or characteristics that significantly identified them as
being at greater risk for severe RSV disease, except for being under 2 years of age.
Human Adenoviruses comprise an important group of etiologic agents
that are responsible for various diseases in adults and children, such as respiratory,
ocular, gastroenteric, and urinary infections. In immunocompromised and organ-transplanted
individuals, these agents can cause generalized infections.
PRINCIPLE
The SARS-CoV-2 Antigen Rapid Test (Nasopharyngeal Swab) is a
qualitative membrane-based immunoassay for the detection of SARS-CoV-2
Nucleocapsid protein in human nasopharyngeal swab specimen. SARS-CoV-2 antibody is coated
in test line region.
During testing, the specimen reacts with SARS-CoV-2 antibody-coated
particles in the test. The mixture then migrates upward on the membrane by capillary
action and reacts with the SARS-CoV-2 antibody in test line region. If the specimen contains
SARS-CoV-2 Nucleocapsid protein, a colored line will appear in test line region as a result
of this. If the specimen does not contain antigens to SARS-CoV-2, no colored line will appear in the
test line region, indicating a negative result. To serve as a procedural control, a colored line
will always appear in the control line region, indicating that the proper volume of specimen
has been added and membrane wicking has occurred.
The Influenza A+B Rapid Test (Nasopharyngeal Swab) is a
qualitative, lateral flow immunoassay for the detection of Influenza A and Influenza B
nucleoproteins in human nasopharyngeal swab specimen. In this test, antibody specific to
the Influenza A and Influenza B nucleoproteins is separately coated on the test line regions of
the test. During testing, the extracted specimen reacts with the antibody to Influenza A and/or
Influenza B that are coated onto particles. The mixture migrates up the membrane to react with
the antibody to Influenza A and/or Influenza B on the membrane and generate one or two colored
lines in the test regions.
The presence of this colored line in either or both of the test
regions indicates a positive result. To serve as a procedural control, a colored line will always appear
in the control region if the test has performed properly.
The RSV Rapid Test (Nasopharyngeal Swab) is a qualitative, lateral
flow immunoassay for the detection of Respiratory Syncytial Virus nucleoproteins in
nasopharyngeal swab specimens. In this test, antibody specific to the Respiratory Syncytial Virus
nucleoproteins is coated on the test line region of the test. During testing, the extracted
specimen reacts with the antibody to Respiratory Syncytial Virus that is coated onto particles. The
mixture migrates up the membrane to react with the antibody to Respiratory Syncytial Virus
on the membrane and generate one colored line in the test region. The presence of this
colored line in the test region indicates a positive result. To serve as a procedural control, a
colored line will always appear in the control region if the test has performed properly.
The Adenovirus Antigen Rapid Test (Nasopharyngeal Swab) is a
qualitative membrane-based immunoassay for the detection of adenovirus antigen in
nasopharyngeal swab specimens. In this test, antibody specific to the adenovirus is separately coated
on the test line region of the test. During testing, the extracted specimen reacts with the
antibody to adenovirus that are coated onto particles. The mixture migrates up the membrane to
react with the antibody to adenovirus on the membrane and generate a color line in the test
line region. The presence of this color line in the test line region indicates a positive
result, while its absence indicates a negative result. To serve as a procedural control, a colored line
will always appear in the control region if the test has performed properly.
REAGENTS
The test contains anti-SARS-CoV-2, anti-Influenza A, anti-Influenza
B, anti-RSV and anti-Adenovirus as the capture reagent, anti-SARS-CoV-2,
anti-Influenza A, anti-Influenza B, anti-RSV and anti-Adenovirus as the detection reagent.
SPECIMEN COLLECTION, TRANSPORT AND STORAGE
Specimen Collection
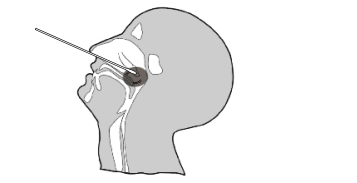
1. Insert a sterile swab into the nostril of the patient, reaching
the surface of the posterior nasopharynx.
2. Swab over the surface of the posterior nasopharynx 5-10 times.
3. Withdraw the sterile swab from the nasal cavity and avoid excess
volume and highly-viscous nasopharyngeal discharge.
Specimen Transport and Storage
Specimens should be tested as soon as possible after collection. If
swabs are not been processed immediately, it is highly recommended the swab specimen
is placed into a dry, sterile and tightly sealed plastic tube for storage. The swab
specimen in dry and sterile condition is stable for up to 24 hours at 2-8 °C.
SPECIMEN PREPARATION
Only the extraction buffer and tubes provided in the kit is to be
used for swab specimen preparation.
Please refer to the Procedure Card for detailed information of
Specimen Extraction.
1. Place the swab specimen in the Extraction Tube with Extraction
Buffer. Rotate the swab for approximately 10 seconds while pressing the head against the inside
of the tube to release the antigen in the swab.
2. Remove the swab while squeezing the swab head against the inside
of the Extraction Tube as you remove it to expel as much liquid as possible from the swab.
Discard the swab in accordance with your biohazard waste disposal protocol.
*NOTE: The storage of the specimen after extraction is stable for 2
hours at room temperature or 24 hours at 2-8 °C.
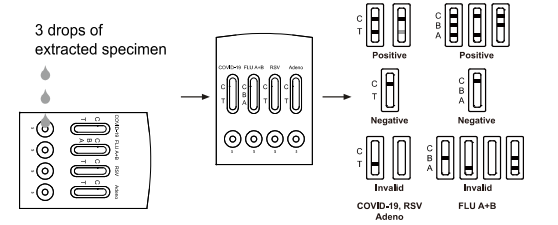
INTERPRETATION OF RESULTS
(Please refer to the illustration above)
SARS-CoV-2/RSV/Adenovirus POSITIVE:* Two colored lines appear in
the SARS-CoV-2/RSV/Adenovirus window. One colored line should be in the
control region (C) and another colored line should be in the test region (T). Positive
result in the test region
indicates detection of SARS-CoV-2/RSV/Adenovirus antigens in the
specimen.
Influenza A POSITIVE:* Two colored lines appear in the FLU window.
One colored line should be in the control region (C) and another colored line should
be in the Influenza A region (A). Positive result in the Influenza A region indicates that
Influenza A antigen was detected in the specimen.
Influenza B POSITIVE:* Two colored lines appear in the FLU window.
One colored line should be in the control region (C) and another colored line should
be in the Influenza B region (B). Positive result in the Influenza B region indicates that
Influenza B antigen was detected in the specimen.
Influenza A and Influenza B POSITIVE:* Three colored lines appear
in the FLU window. One colored line should be in the control region (C) and two
colored line should be in the Influenza A region (A) and Influenza B region (B). Positive result
in the Influenza A region and Influenza B region indicates that Influenza A antigen and Influenza
B antigen were detected in the specimen.
*NOTE: The intensity of the color in the test line region (T) will
vary based on the amount of SARS-CoV-2 antigen, Influenza A and/or B antigen, RSV antigen,
Adenovirus antigen present in the specimen. So any shade of color in the test region (T/B/A)
should be considered positive.
NEGATIVE: One colored line appears in the control region (C). No
apparent colored line appears in the test line region (T/B/A).
INVALID: Control line fails to appear. Insufficient specimen volume
or incorrect procedural techniques are the most likely reasons for control line failure.
Review the procedure and repeat the test with a new test. If the problem persists, discontinue
using the test kit immediately and contact your local distributor.
Order Information
| Cat. No. | Product | Specimen | Pack |
| ICIC-525 | COVID-19 and Influenza A+B Antigen Combo Rapid Test | Nasopharyngeal Swab | 20T |
| ISIR-535 | COVID-19/Influenza A+B/RSV Antigen Combo Rapid Test | Nasopharyngeal Swab | 20T |
| IRT-545 | COVID-19/Influenza A+B/RSV/Adenovirus Antigen Combo Rapid Test | Nasopharyngeal Swab | 20T |
| IRT-555 | COVID-19/InfluenzaA+B/RSV/Adenovirus /M.pneumoniae Antigen Combo
Rapid Test | Nasopharyngeal Swab | 20T |
| ISIC-525 | SARS-CoV-2 and Influenza A+B Antigen Combo Rapid Test | Nasopharyngeal Swab | 20T |








